Appelez
+212 0522274820+212 0522276640
+212 661134182
Il sagit d'une affection douloureuse périnéale qui survient généralement à partir de la quarantaine, avec prédominance féminine (2/3 des cas).
Cependant elle n'épargne souvent pas au voisinage de 30 ans.
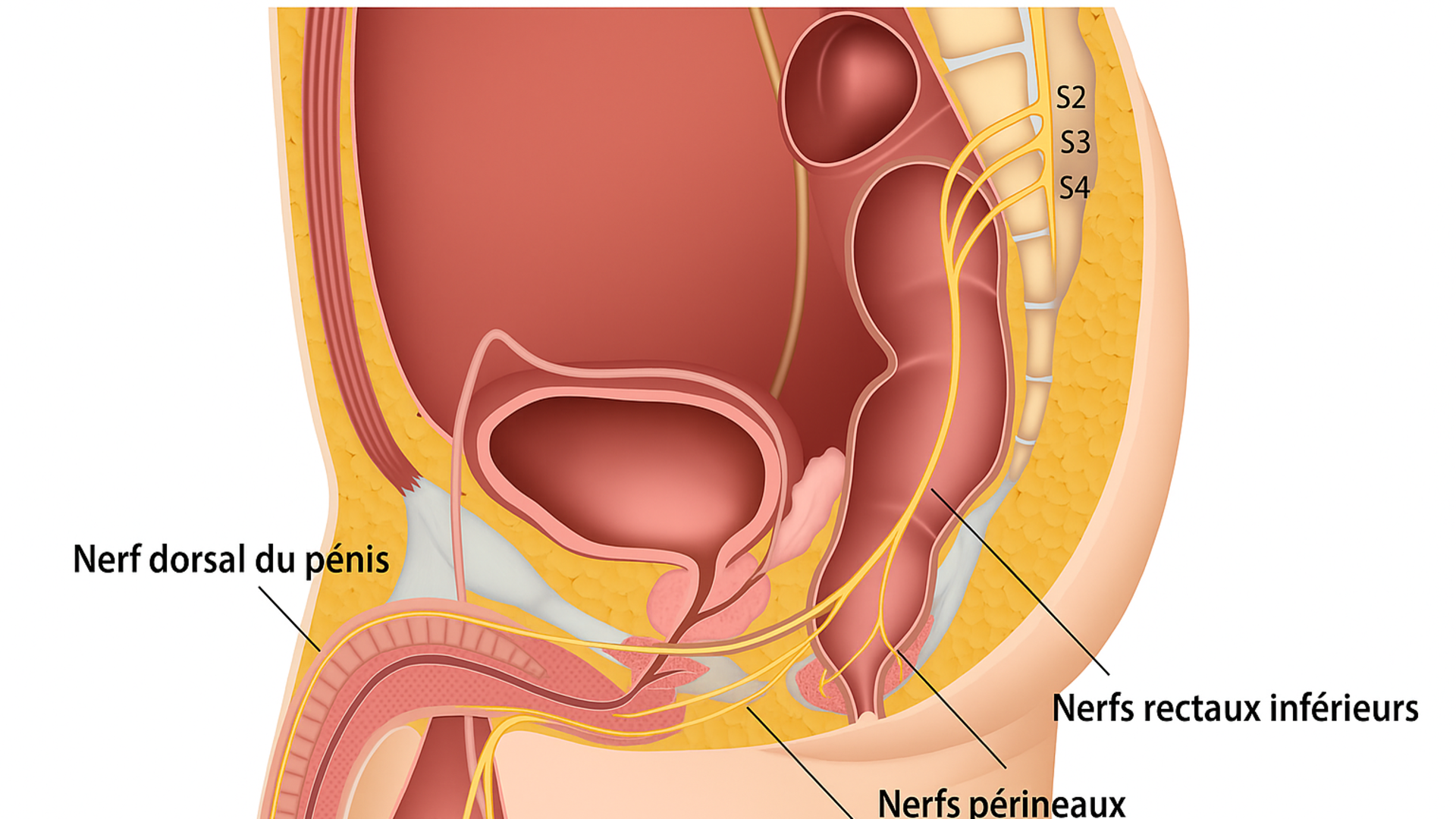
Le nerf pudendal est un nerf sensitif moteur végétatif. Il sort de la moelle épinière à la région la plus basse (périnée).Ce nerf domine et 'gouverne' le périnée. Il a un passage obligé qui longe le petit bassin, s'insère entre deux ligaments:
le ligament sacro épineux et le ligament sacro tubéral, et puis rentre dans un canal fibreux (canal d'Alcock) après il va donner 3 branches: le nerf périnéal, le nerf dorsal de la verge chez l'homme ou nerf dorsal du clitoris chez la femme et le nerf rectal inférieur.
Ce nerf peut être serré dans son passage, il va souffrir de cette striction. Les branches de division qui en proviennent souffrent aussi ainsi que les organes et les muscles qu'elles innervent.
C'est ce qui constitue la névralgie pudendale caractérisée par une douleur qui va du pubis l'anus. Son diagnostic est éminemment clinique et tous les examens faits se révèlent normaux. Les douleurs sont exacerbées à la position assise, calmées à la position allongée. A type de brûlures de décharges ou de Pesanteur avec sensation de corps étranger intravaginal ou intrarectal.
Déclenchées par l'examen clinique qui au toucher vaginal et/ou rectal va provoquer une douleur à l'identique.
La preuve du diagnostic peut être apportée par le bloc test qui consiste en une infiltration échoguidée ou mieux scano guidée par un produit anesthésique associé ou non à un corticoïde. Le résultat est immédiat.
Cette pathologie est peu connue des médecins ce qui amène à l'errance diagnostique et à la psychiatrisation de la maladie avec pour conséquence le retard au diagnostic.
Plusieurs traitements sont proposés: médical, physiothérapie, chiropraxie, radiofréquence, cryo neurolyse dotés d'un effet transitoire, plutôt d'un effet placebo.
Mais les plus efficaces sont :
Le traitement médical adapté à chaque cas et bien conduit.
Téléphone
+212 0522274820
+212 0522276640
+212 661134182
contact@medicinterfacemaroc.com
Adresse
12, Boulevard d'Anfa, Casaclanca - Maroc

Votre partenaire de confiance pour des soins médicaux de qualité au Maroc. Nous nous engageons à offrir des services de gestion et de suivi adminitratif tout le long de votre séjour au Maroc.
+212 0522274820
+212 0522276640
+212 661134182
contact@medicinterfacemaroc.com
12, Boulevard d'Anfa, Casaclanca - Maroc
© Medic Interface Maroc. Tous droits réservés.
Conçu par modiom Tech
